
Transjugular Intrahepatic Portosystemic Shunt (TIPS)
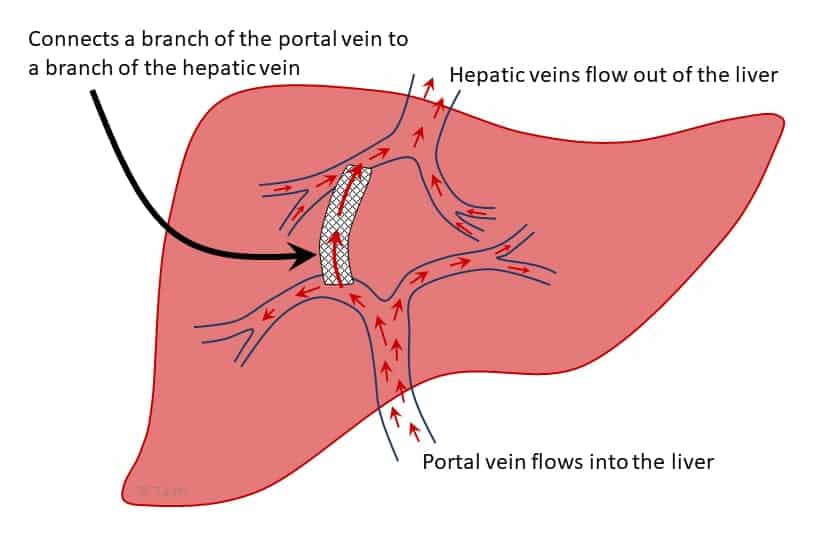
A TIPS relieves the high blood pressure in the portal vein (called portal hypertension) that often occurs in the setting of liver cirrhosis. A TIPS allows blood flowing into the liver from the portal vein to flow through the TIPS stent directly into the hepatic vein, the vein that drains blood out of the liver to the vena cava and then immediately into the heart.
Why would a person need a TIPS?
The two main reasons that a person might need a TIPS are:
- Ascites (fluid accumulation in the abdomen) that cannot be managed with dietary sodium restriction and diuretics (“water pills”). Sometimes ascites crosses the diaphragm muscle between one of the lungs and abdomen to fill the space around the lung, typically the right lung. This is called hepatic hydrothorax and TIPS can often help this as well. TIPS should not be considered if the fluid accumulation can be controlled by dietary sodium restriction and diuretics.
- Bleeding from varices (swollen veins, usually in the esophagus) that cannot be controlled with endoscopic treatment such as rubber band ligation. Bleeding varices in the stomach, rectum or elsewhere are more difficult to treat with rubber band ligation and a TIPS is often needed in these situations.
How is a TIPS inserted into the liver?
A radiologist with special training places the TIPS by going through a jugular vein in the neck and straight down into the liver. People are usually heavily sedated or asleep with general anesthesia for the procedure. After numbing up a spot in the skin over the jugular vein on the side of neck (typically the right side), a catheter like a large IV is temporarily placed through the skin into the jugular vein. A partially covered stent is inserted through the catheter, which is passed down through the superior vena cava, right atrium of the heart, inferior vena cava, into the hepatic vein and through the liver into the portal vein. The TIPS stent is very narrow when it is inserted, and it is passed into the liver over this device. It is expanded once it is in the liver with one end in a branch of the portal vein and the other end in a branch of the hepatic vein. Sometimes more than one stent is placed in a row to bridge that distance. At the end of the procedure, the catheter in the neck and the device used to place the shunt are removed. Just the TIPS stent is left in the liver and a small bandage is placed on the neck.
Can a TIPS be removed?
No, a TIPS cannot be removed. If the flow through the TIPS is greater than anticipated which reduces blood flow to the rest of the liver too much, its diameter can be reduced. This is called a TIPS revision.
What are the risks of having a TIPS?
One of the major functions of the liver is to remove toxins from the blood such ammonia and other toxins absorbed from the colon, so when a TIPS is placed, the blood going into the liver is not filtered as well. An increase in the blood levels of ammonia and other toxins can cause confusion, disorientation and even coma. This is called hepatic encephalopathy. Taking a medication called lactulose helps flush the toxins out of the colon and another medication called rifaximin reduces the amount of toxins produced in the colon. These are sometimes needed after a TIPS. If a person is already taking those medications, then a TIPS may not be a good option because there are no additional treatment options if hepatic encephalopathy occurs after a TIPS.
Other risks of having a TIPS include liver infarction which is when some of the liver dies because of a lack of blood flow, and also disruption of the bile ducts, bleeding from the liver into the abdomen, and infection. Fortunately, these are all rare events.
The decision to have a TIPS requires a careful consideration of the potential benefits and whether these benefits outweigh the risks.
What happens after a TIPS?
Immediately after a TIPS, people are typically kept in the hospital, sometimes in the ICU for a night, for close monitoring for signs of bleeding. People typically go home a day or two after a TIPS.
After going home, people with a TIPS should be monitored closely for signs of hepatic encephalopathy. This may not occur for a week or two after the TIPS was inserted and can cause confusion and disorientation. The hepatologist caring for the person should be notified immediately if this happens. People with evidence of hepatic encephalopathy should not drive or engage in activities that could be a danger to themselves or others (physically or financially).
Diuretic doses typically need to be reduced after a TIPS while monitoring for signs of re-accumulation of fluid or dehydration and impaired kidney function. Any dizziness or other signs of dehydration should be reported immediately to the hepatologist.
TIPS occlusion, or blockage, can occur within days, weeks or even years after a TIPS. This is caused by blood clotting in the TIPS or reduction in the TIPS diameter due to the excessive scar tissue in the liver. The TIPS is typically reevaluated periodically by ultrasound to confirm its adequate function. If it becomes narrowed or fully blocked, an interventional radiologist may need to reopen it.
What are the common reasons that a person cannot have a TIPS?
The major reasons why a TIPS should usually not be placed are:
- The liver function is so poor that TIPS can cause further liver failure. Usually an INR above 2.0, or total bilirubin above 3 to 5 mg/dl predicts poor outcomes. Once the MELD score is above 15, a TIPS has a higher risk; it is generally not done if the MELD score is more than 18-20 unless it is needed in an emergency to control bleeding from varices and the person is on a liver transplant list.
- The right side of the heart, the side that pumps blood through the lungs, is not strong enough to handle the increased blood flow, or if there already is severe hypertension in the lung circulation because the increased flow from the TIPS can cause severe strain on the heart. This is commonly determined by an echocardiogram prior to TIPS placement
- The portal vein is blocked by a blood clot (portal vein thrombosis).
- The presence of liver cancer or other types of cancer within the liver.
- TIPS is generally not considered to treat large varices in esophagus or stomach if they have never bled.
What are the alternatives to having a TIPS?
For people who have a TIPS to control ascites (abdominal fluid) or hepatic hydrothorax (ascites that crosses the diaphragm muscle into the chest cavity and causes the lung to shrink), typically the only alternative is to continue to have fluid removed by paracentesis (from the abdomen) or thoracentesis (from the chest cavity). In end-of-life situations where palliative care is appropriate, a drain can sometimes be left in place and used to periodically withdraw fluid from the chest or abdomen. This is not done routinely because of the risk of infection and the continuous loss of protein in the fluid that is removed.
Information provided with the help of…
Brent A. Tetri, MD
Professor of Internal Medicine
Division of Gastroenterology & Hepatology
Saint Louis University
Kamran Qureshi, MD
Associate Professor of Internal Medicine
Division of Gastroenterology & Hepatology
Saint Louis University
Last updated on August 17th, 2023 at 01:58 pm